What is the structure and function of the testicles?
Male sex organs are classified into two types: those that can be seen from the outside and those that are inside. Only a sac (scrotum), which contains the penis and testicles, is visible from the outside. Inside, there are the testicles in the sac, the epididymis where the sperm obtain the ability to travel,
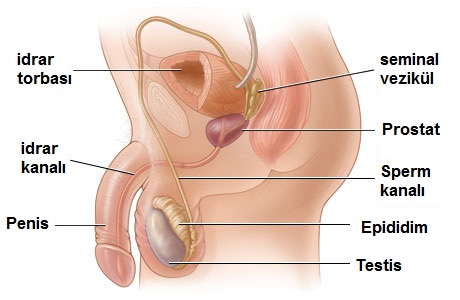
a sperm canal (vas deferens) that enables the sperm to discharge into the urinary canal, the seminal vesicles that contribute to the production of semen and the prostate.
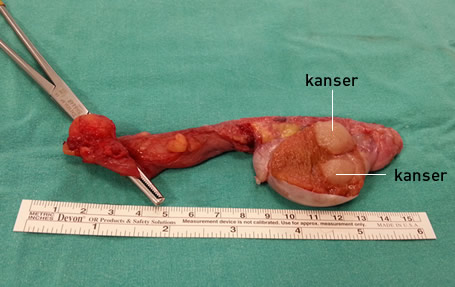
In an adult male, there are 2 testicles, each measuring approximately 4 cm in length and 3 cm in width. The testicles are in charge of sperm development as well as testosterone production, which is a male hormone. Testosterone hormone works while the baby is still in the womb and provides the development of the male organs, as well as the development of the male body structure, male pattern hair growth, and the growth of the sexual organs during puberty. In order for the testicles to perform these functions well, they must be in an environment 1-2 degrees colder than body temperature. Therefore, unlike women, male eggs are outside the body, in other words they are inside a sac (scrotum) hanging from the body. When the testicles are split down the middle, several thin canals appear, similar to the inside of a fig fruit, and have a soft consistency.
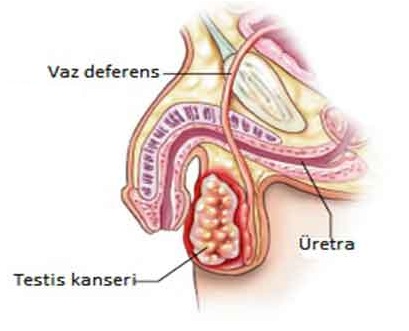
What is testicular cancer?
There are many cell types in the testicle such as sperm-producing cells (sertoli cells), testosterone-producing cells (leydig cells), sperm themselves, blood vessel cells, nerve cells, lymph cells, fat cells, and connective tissue cells. In testicular cancers, if abnormal proliferation occurs in these cells in the testicle for some cause, a mass forms here, just as it does in cancers of other organs. These cells differ from normal cells in that they gradually proliferate, develop massively, and then spread to other organs in the body and surrounding organs through blood and lymph vessels, eventually forming cancer in those organs. This condition is called spreading or metastasis.
Cancer that develops in the testicle is named according to the cell from which it originated. More than 90% of testicular cancers originate from testicular cells. Aside from that, there are different cancers such as lymphatic cancer and fat cancer.
Naming, treatment, and follow-up protocols of testicular cancers vary widely. One of the testicular cancers (SEMINOMA) is different from all other types. It is more common and responds very well to treatment. Furthermore, it is only cancer for which radiation therapy is effective. Therefore, this cancer is examined under a separate heading from others. Hence, testicular cancers are divided into two as seminoma and others.
What causes testicular cancer?
Why testicular cells proliferate abnormally and what triggers this is still unclear. However, some risk factors have been determined based on the collective data of thousands of patients diagnosed with cancer. While having these risk factors does not guarantee that cancer will develop, not having them does not rule out the possibility of cancer developing. Testicular cancer is common in 20-40 years of age. Aside from that, the risk factors listed are as follows.
- – History of undescended testicles,
- – Klinefelter syndrome (a genetic disease),
- ⁃ Testicular tumor in family (first degree relatives),
- – Tumor or potentially tumorigenic cell (TIN) in the contralateral testis,
- – Infertility.
What complaints do testicular cancers cause?
Testicular cancers are often noticed by the patient in the early stages, but most patients are embarrassed to talk about a problem with their genital area or to have it examined, so they consult a doctor too late. In Turkey, the average application process takes 5 months. However, testicular tumors are very rapidly spreading tumors and diagnosis at an early stage is life-saving. However, at the time of application, many patients’ testicular tumors had already spread across their bodies.
Unless proven otherwise, all masses, swellings, and abnormal structures discovered in the testicle should be treated as tumors, and a prompt evaluation should be made. There are many other reasons that cause swelling or mass in the testicle and these should be distinguished as soon as possible.
The first complaint would be a mass in the patient’s scrotal sac, based on this knowledge. Although this mass does not normally cause pain, it has a 15% risk of being painful. Apart from this, if the tumor has metastasized, there may be complaints due to problems developing in the organs where the tumor has spread. These may be cough, low back pain, swelling in the legs, abdominal pain, neck pain, etc. due to lung involvement.
How is testicular cancer diagnosed?
The first step in making a diagnosis is taking a comprehensive medical history and doing a thorough physical examination on the patient. An experienced urologist can often distinguish on palpation whether the mass in the testicle is malignant (cancer). Because mostly, tumors in the testicles are painless. Furthermore, the testicle has a soft consistency and a smooth surface, while the tumors that develop next to it have a very rough and irregular surface. Yet, other benign masses in the scrotal sac are generally not very rough and their surfaces are regular. However, sometimes the tumor is accompanied by inflammation (orchitis), making examination difficult and the tumor difficult to distinguish.
In any case, blood tests and ultrasonography should be performed for all patients with suspected testicular mass. Ultrasonography does not contain radiation and is an inexpensive method available in almost all hospitals, and it is about 95% helpful in diagnosis. In the blood sample, 2 hormones produced from tumor cells are examined. These are beta-HCG and alpha-fetoprotein ‘(AFP). However, since one of these hormones increases in some tumors and the other in other tumors, there are also tumors where both increase or decrease at the same time. Therefore, if these analyses show an increase, it supports the tumor diagnosis, but a low level does not rule out the possibility of a tumor.
Since most of the testicular tumors are caught in the late stage, it is not enough to determine the mass in the testicle by just looking at the sac. Lymph nodes and other organs in the abdominal area where the tumor would first reach should also be scanned in these patients. This scan is usually done by Computed Tomography (CT).

How are testicular cancers treated?
Regardless of the stage (early or spread), the patient with a tumor in the testicle should be operated on immediately (within 1-2 days). The aim of this surgery is to remove both the testicle and the mass. Thus, both the early-stage patient is rescued from the disease and the final tumor diagnosis is made. We obtain this diagnosis as a result of the pathological examination. It is determined in the pathology report from which cell the tumor originates (that is, its type), whether it is aggressive, and whether it has spread to its surroundings. The surgery is performed with an approximately 3 cm incision from the inguinal region. The testicle is cut through this incision and removed together with its canals.

After this stage, it is checked whether the tumor has spread to distant areas with the CT mentioned above. In other words, the stage of the disease is investigated. The following treatments are decided according to the stage and type of tumor.
Stage 1: The tumor is only in the testicle
Stage 2: Tumor has spread to lymph nodes in the abdominal area
Stage 3: The tumor has spread to lymph nodes near the lung and/or to the lung.
Stage 4: The tumor has spread to other organs other than the lung (Brain, bone, liver, etc.)
In many testicular tumors, even if the patient is in stage 1, additional drug therapy (chemotherapy) or radiation therapy (radiotherapy) is required. An additional treatment is definitely applied to the patient who is in stage 2. While this treatment is Radiotherapy for tumors called seminoma, it is Chemotherapy for those other than seminoma. Chemotherapy is applied in stages 3 and 4. Patients with testicular tumors are monitored for many years, and the tumor may recur after subsequent treatments.